Jungian Essays
On illness as opening, the symptom as symbol, and the discipline of reading the wound
The medieval Wound Man stands annotated because the physician understood the wound as a site of knowledge before it was a site of damage. Drawing on Meier's tertium, Jung's psychoid, and the clinical writings of Bucci, McDougall, Ulanov, and Schwartz-Salant, this essay reads psychosomatic illness as the body's symbolic language, the symptom as a symbol that has not yet been received, and the wound as an aperture through which something from the deep structures asks to be recognized.
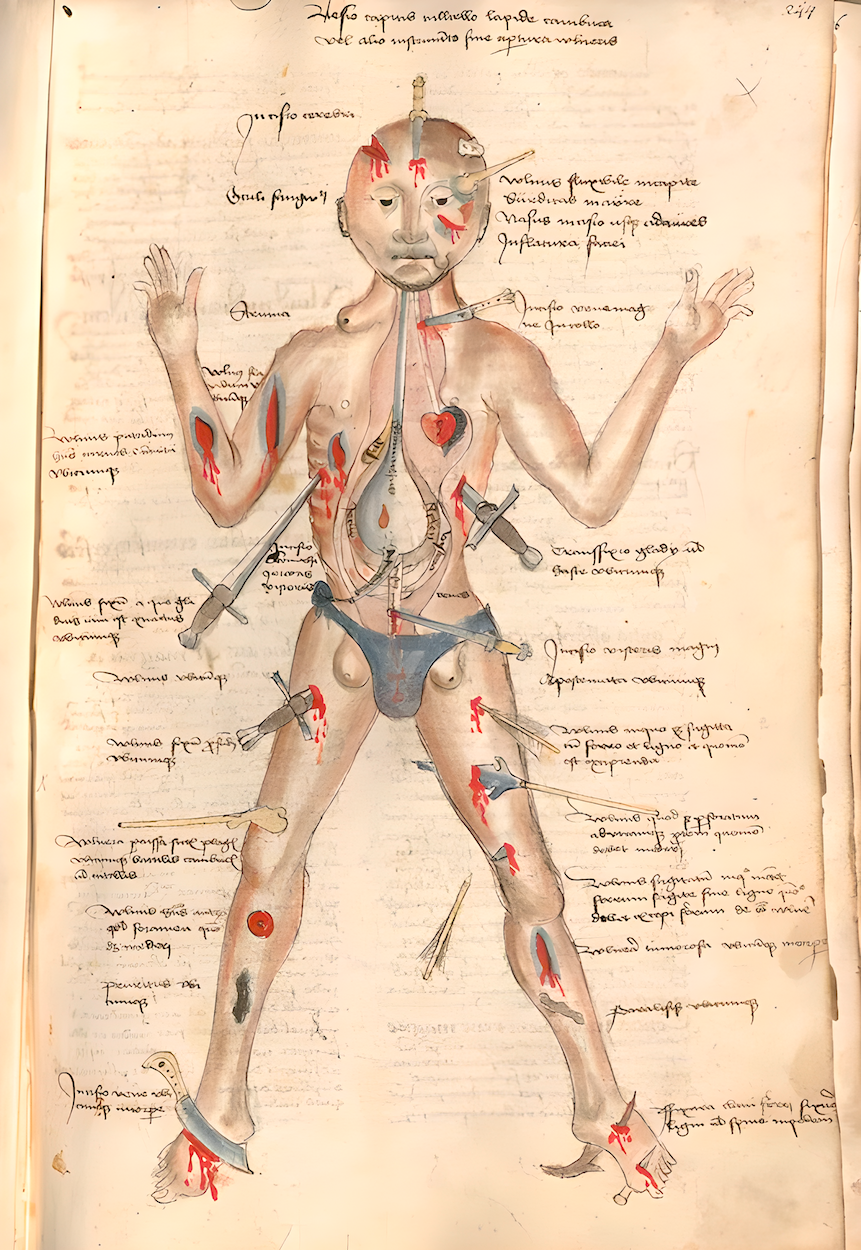
In fifteenth-century surgical manuscripts, an intriguing figure appears that has no name in the historical record but has acquired one by convention: the Wound Man. It depicts the torso of a naked figure marked by various incisions, cuts, and lacerations. Weapons of the era, such as knives, lances, arrows, and swords, are shown piercing the body. An annotation appears beside each wound, forming a visual table of contents. Although instructional in purpose, the image carries a macabre quality. It gathers into one body every injury a medieval surgeon might be called upon to treat.
As we look at the imagery of the Wound Man’s injuries, let us pause for a moment to consider the bleeding openings themselves. Etymologically, the word “wound” comes from Old English wundian, meaning a breach—in this case, a breach in physical tissue. As we look at the illustration, we are faced with its double meaning: the wound is both an opening and a gateway that must be studied and understood.
Within the past few centuries, we have considerably refined—and in many cases even perfected—the treatment. However, what we have lost is the practice of "reading" the wound. Despite our convinced awareness of the connection between mental and physical life, we have lost the ability to truly listen to and understand our bodies. We still approach symptoms as something to be resolved rather than read, as a malfunction rather than a form of communication.
Our ailments and diseases are openings through which something powerful and vital seeks to emerge from the deep structures of the body into conscious awareness. A habitual tendency to treat illness as a malfunction, something to be eliminated, can itself become a mechanistic attitude that sometimes brings on the illness in the first place. We need to complement this survivalist approach with something just as essential: the ability to penetrate into the archetypal stories embedded in our wounds.
The correlation between emotions and illnesses is now common knowledge. Popular psychology has given us a rather elaborate vocabulary for mapping illness onto emotion: this emotion causes that illness, an unresolved conflict produces that symptom, stress explains the rest. The appeal of such a vocabulary is understandable and, at times, even useful. However, such a dictionary can miss the point: the specificity of what your own body is carrying. More precisely, it can cause you to overlook your own unfolding story.
The same wound can open onto entirely different inner stories in two different people. Chronic back pain in one person may be quite different from chronic back pain in another. A diagnostic key that maps emotion to illness will miss precisely what is specific, which is also what is meaningful. This reductionism has a mechanical quality and abruptly stops the symbolic understanding of illness before the psyche can produce any meaningful integration.
We should briefly mention the term somatization. Ford defines it as "a process by which the body (the soma) is used for psychological purposes or for personal gain." Clinically, it refers to bodily processes used to express displaced emotions and symbolically enact what cannot be spoken. However, the archetypal undercurrents can be missed entirely.
The paradigm of reading our wounds as sites of meaning does not diminish the value of systematically understanding ailments. It is not opposed to it. But we should not confuse meaning-making with triage management.
LP · NCPsyA · SCPsyA
Jungian psychoanalyst practicing in New York's West Village. This journal presents original essays on depth psychology, dreams, and the inner life.

Carl Meier, a Jungian analyst, discussed the shared etymology of two notable words: symbol and symptom. Both derive from the common root sym, which denotes the “meaningful coincidence of at least two distinct magnitudes”. According to ARAS, that common root sym symbolizes “the throwing together of a thing and its meaning, and is warning and portent, somatic analogy of psychic conflict”.
The medical vocabulary of antiquity carried a philosophy of illness that differs structurally from the modern causal model: the symptom coincides with the symbolic meaning of illness (coincidentia in Latin), rather than reflecting a cause-and-effect relationship. Meier goes on to say that this idea is essentially the same as what Jungian psychology calls synchronicity. It assumes the existence of a third element, or tertium, something that stands above both body and psyche. He suggests that healing can occur only when this higher-order third factor is constellated, namely, a symbol or archetype representing wholeness.
In a sense, a symptom is a symbol that has not been accepted. The somatizing patient is no less imaginative than anyone else, but his psyche uses the body to produce symbols in the only form available to him.
Wilma Bucci offers a formulation that reorients the entire clinical picture. Rather than viewing a physiological symptom as a malfunction or a pathology to be corrected and eliminated, she interprets it as a healing gesture, an attempt at symbolization:
“Somatic or psychic symptoms may carry out a progressive symbolizing function, in the same sense as dreams and fantasies, where other symbols are not available to be used. Symptoms, like dreams, are fundamentally attempts at symbolizing, healing in the psychic domain, although symptoms may then bring new problems of their own.”
The question then becomes: what kind of psychic material bursts through the soma? What is the message the unconscious is trying to transmit in the form of an illness?
Ann Bedford Ulanov describes physical maladies as “unlived psychic afflictions” that arise from a person’s inability to consciously experience an emotional process. For example, instead of facing sorrow and grief, a person may develop “weeping sores of the body”.
In her book Theatres of the Body (1989), Joyce McDougall connects somatic ailments with early developmental failures. For some patients, the "silent" expressions of emotion in early childhood result in alexithymia, the difficulty of processing or describing one's emotions, and the somatic problems later in life are “psychic dramas” the body is left to stage.
Some patients describe their physical suffering as a state with no image attached to it, just pain and dread that seem to have no end. Schwartz-Salant names these "non-metabolized states occurring with no images, just pain and terror at their seeming endlessness."
If we allow ourselves symbolic thinking and ask, “What part of me is ailing? Which archetype in me is trying to tell me its story?”, then we begin to understand our maladies in their depth.
For some people who struggle most to relate to images and dreams, the body becomes the repository of metaphoric language, and bodily afflictions become symptoms-as-symbols, the primary means of communication between the conscious and the unconscious.
Here we need to clarify an important divergence in the interpretation of drive theory as understood by Freud and Jung, and how it relates to the image.
Freud’s model is essentially hierarchical. Instinct is primary, biological, a drive pressing for discharge. The image, fantasy, dream, and symbol are derivatives. They are what the drive looks like after passing through the mind’s apparatus. The image reflects instinct, represents it, and gives it a psychic form. In this model, psychology is ultimately a function of biology.
This divergence became explicit with Jung's 1912 Symbols of Transformation, in which he reconceived libido as undifferentiated psychic energy rather than as Freudian drive. Jung ultimately refused Freud’s hierarchy.
For Jung, the image was not a representation of the instinct, but rather another facet of it. The instinct has two aspects simultaneously: a somatic aspect, which is the drive, the bodily pressure, the compulsion to act, and a psychic aspect, which is the image, the fantasy, the symbolic form that the instinct takes in the imagination. Neither is more primary than the other, neither is a derivative of the other: they are two co-equal faces of one process. As Samuels puts it, “instincts and images have the same psychoid root”.
Another important aspect of Jung’s idea of the psychoid region is that it refers to “the transconscious areas where psychic processes and their physical substrate touch”. Therefore, communication between image and soma is bidirectional, creating a powerful gateway for potential transformation.
If we follow at the implication of this etymological argument further, the conclusion is this: if symptom and symbol share a common root, then that root signifies the “falling-together” (coincidentia) of distinct magnitudes rather than the discharge of one into the other. This means that the relationship between psyche and soma in psychosomatic illness is not causal. Rather, psyche and the somatic event occur together because something beneath them both is in motion.
Meier calls it the tertium: a third factor of “a higher order” than either body or psyche, the archetypal pattern of which both events are simultaneous expressions. In Jungian terms, the tertium approximates the archetype of totality, or the Self. The somatic symptom and the psychic conflict are two aspects of a single constellation, linked not by causation but by a common origin in an archetypal process that neither can name on its own.
The clinical consequence is significant. If the psyche-soma relationship were causal, treatment would mean resolving one to dissolve the other: resolve the psychic conflict and the body would heal, or treat the body and the psychic disturbance would resolve. Anyone who has worked clinically with somatizing patients knows it does not work this way. The interpretation that ought to dissolve the symptom does not always do so. The medication that ought to heal the body sometimes silences the symptom without addressing what it was expressing, only for the patient to develop a symptom elsewhere in the body because the tertium has not been addressed.
In Meier’s view, healing proceeds neither through somatic intervention alone nor through psychic interpretation alone, but through the constellation of the archetypal pattern that both events express. The symbol of totality must be brought into view. This is what makes the wound, in Jungian work, something other than a problem to be eliminated. The wound is an invitation. It is the place where the tertium asks to be recognized: look here, the symptom says, this is where the unrecognized whole is trying to surface. Stop and ask why you feel this way.

In shamanic traditions across cultures, the call to heal often begins with illness. The future shaman falls into a sickness no ordinary remedy can reach. Anthropological accounts often describe this illness as an initiatory process, an intense psychological and physiological descent that can approach death itself. This territory must be known and integrated, and the knowledge gained there gives the shaman the authority to treat others, since their own suffering shows that they were not exempt.
Greek mythology embodies this archetype, known as the wounded healer, in Chiron, the centaur who taught medicine to Asclepius. Wounded by a poisoned arrow that could not kill him because he was immortal, Chiron was condemned to bear a wound that would never heal. From that wound came his knowledge of healing and his ability to attend to the suffering of others, because the territory of suffering was no longer foreign to him.
Jung returned repeatedly to this myth, sensing its importance for clinical psychology. Like Chiron, the analyst is bound to the figure of the wounded healer, for without having suffered, he cannot truly reach a wounded patient. His interpretations will be heard as instruction rather than recognition. In both analyst and patient, the wound opens a transformational space of suffering where one psyche can meet another.
The serpent on Asclepius’s staff embodies this idea of polarity. At one end, it represents cold-blooded instinct: the body’s intelligence operating beneath conscious will, a creature that moves without thought. At the other, it is an image of wisdom at its deepest level. And those two ends are forever intertwined: what the body knows from below, the Self knows from above.
This understanding gives the wound a telos beyond the traditional expectation of cure. Acting as the body’s Shadow, it is something to be understood rather than removed, for it holds information that consciousness cannot yet bear. The somatic symptom becomes the point at which wholeness tries to assert itself against a one-sided conscious attitude, and the body will continue to insist on this until the ego comes into relation with it.
Many patients bring health concerns into the consulting room alongside emotional ones. When that happens, both analyst and patient face the dilemma of how to approach these two aspects of suffering. The temptation is often to defer the body to medicine and the psyche to talk therapy, as though the two could be addressed separately. But if the symptom and the symbol in fact “coincide” around a common center, then the analyst’s task is neither to interpret the symptom away nor to leave the body to its own devices, but to hold both sides until the tertium begins to constellate.
Separating body and psyche into the distinct domains of medicine and therapy can create a dangerous situation in which one face of the archetypal process is addressed while the other is left unattended. Verena Kast names this risk clearly:
“One danger of psychotherapy is that it becomes too “mental” (wordy) and loses the link with the body. When this happens, psychotherapy loses the psyche also. Correspondingly, a danger of pure bodywork is that it may release much somatized energy without this raw affect becoming available to the mind in the form of images or words that would enable it to be understood.”
Jungian analyst Marion Woodman, drawing on her own long history of illness, developed a simple practice that illustrates what bidirectional translation looks like. She placed images from her dreams in the afflicted areas of the body. It was her way of bringing the mind into contact with the body exactly where the body was trying to be heard. Communication goes both ways: the body can produce a symptom that draws the mind’s attention, and the mind can produce an image that the body can take in.
This reframes what we mean by healing in the first place. As Meier says, “symptoms are healed every day in the offices of doctors of all sorts, and are set down as cured by doctor and patient alike”. Many of them do not return; many return in another form. Meier observes that what Jung means by healing is something other than the “healing of symptoms”. What he meant was closer to transformation: the patient comes to understand the meaning of the suffering, the place of the illness in “the totality of the patient’s life”, what was being asked through the wound. The wound has to yield a meaning, and the causa finalis, the purpose behind the suffering, has to come into view.
In depth psychology, the wound is a transformational symbol. The Wound Man stands annotated because the medieval physician understood that the wound was a site of knowledge before it was a site of damage. The work of an analytic life is to relearn that practice with our own wounds—slowly, and with the attention they deserve.
LP · NCPsyA · SCPsyA
Jungian psychoanalyst practicing in New York's West Village. This journal presents original essays on depth psychology, dreams, and the inner life.
These images are not mere metaphors. They are lived experiences. Analysis is how you learn to navigate them.

Schedule a free initial consultation. There is no commitment — only the opportunity to explore whether depth work is right for you.



